Resource implications and budget impact of managing cow's milk allergy in the UK
Cow's Milk Protein Allergy (CMPA) is an immune reaction to the protein in cow's milk and generally develops in infancy, with an estimated incidence of 2-3% in the western world. Presenting symptoms can include eczema, urticaria, wheezing, swelling, gastrointestinal (GI) and a range of other symptoms.
Key points
This is the largest study ever undertaken in CMPA, based on 1,000 infants followed for 1 year..
It suggests GPs play a greater role in CMPA management in the UK than previously thought, with a majority of cases diagnosed and treated by GPs.
During the study, 76% of infants under 6 months of age were initially prescribed soy by their GP, contrary to current guidelines.
CMPA imposes a high burden on NHS resource. Schemes to reduce time to treatment, time to diagnosis and time to symptom resolution could decrease this burden.
Background
Cow's Milk Protein Allergy (CMPA) is an immune reaction to the protein in cow's milk and generally develops in infancy, with an estimated incidence of 2-3% in the western world. Presenting symptoms can include eczema, urticaria, wheezing, swelling, gastrointestinal (GI) and a range of other symptoms.
Clinical nutrition preparations are useful treatments for infants with CMPA and include soy-protein-based milk, extensively hydrolysed formulas (eHF) or amino acid formulas (AAF).
Where available, guidelines generally suggest soy formula or eHF for sufferers aged over 6-months, but initially only an eHF for those under 6-months old. Infants who cannot tolerate soy are generally switched to an eHF; those who cannot tolerate eHF should be switched to an AAF.
Food allergies such as CMPA represent an important source of morbidity and healthcare utilisation, so a health economic study on CMPA in the UK is warranted.
Aim of study
To determine: how infants with CMPA are managed in UK clinical practice, including assessment of time to symptom resolution; associated resource implications and budget impact for the NHS.
Methodology
A computer-based model stratified CMPA patients according to presenting symptoms and outcomes. Resource utilisation was quantified for each strata and unit resource costs (2006/07 prices) were applied to estimate 12-monthly healthcare costs and consequences of current clinical practice for CMPA.
Study population included 1,000 randomly selected infants from the THIN database, given a Read code for CMPA in their medical history and at least one prescription for a clinical nutrition preparation and registered with their GP for at least 12 months after first consultation for this problem.
Results
For the study cohort, mean age at presentation to GP was 3.2 months (95% CI: 3; 3.4) and 45% were female.
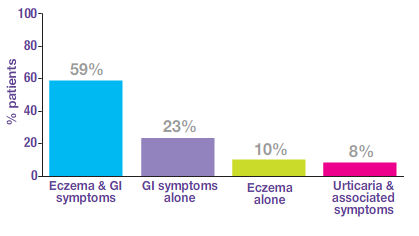
Presenting symptoms
Treatment patterns
CMPA treatment varied according to presenting symptoms. Number of patient pathways ranged from 1 for those with anaphylaxis, to as many as 16 for those with combined eczema/GI symptoms.
Mean time from initial presentation to first prescription for a clinical nutrition preparation was 2.2 months (95% CI: 2; 2.3).
Soy was the initial clinical nutrition preparation of choice for the majority, with 60% of all infants in the cohort initially treated with soy, 18% with eHF and 3% with AAF.
56% were <6 months old at start of treatment; contrary to guideline advice, 76% of them were given soy. 21% in this age-group were initially given an eHF; 3% received an AAF.
A mean of 9% of patients remained symptomatic on soy and 29% on eHF. In such cases, patients were considered intolerant to the prescribed preparation and switched to a different one.
Symptom resolution and clinician visits
All patients became symptom-free during 12 months follow-up, after receiving a clinical nutrition preparation. Time to symptom resolution from initial GP visit was a mean of 2.9 months (95% CI: 2.8; 3).
It took a mean of 3.6 months (95% CI: 3.4; 3.7) to make a formal diagnosis from the initial GP visit. Patients underwent very few blood tests or skin prick tests, suggesting GPs used symptom resolution as a marker for clinical diagnosis.
GPs made the diagnosis in 86% of cases and specialists in the remainder.
In the 12 months following initial presentation, patients had a mean 18.2 visits (95% CI: 17.5; 18.9) for CMPA.
Healthcare costs and budget impact
Overall, 12-monthly NHS costs following initial presentation to GP was estimated at £1,381 per patient (95% CI: £1,115; £1,649).
In 2006 in the UK there were 734,000 live births; assuming a 2.5% incidence of CMPA, an estimated 18,350 infants per annum can be expected with new-onset CMPA. The study model allows calculation of a total NHS cost of £25.6 million for managing 18,350 infants with CMPA over 12 months following presentation to a GP, with resource-use including:
- 336,575 visits to a GP (99.5% CI: 333,675; 339,474),
- 12,443 outpatient visits (99.5% CI: 11,992; 12,894),
- 1,203 hospital admissions (99.5% CI: 919; 1,483).
Date of preparation: August 2010
- Stadkevicius E, Nagy E, Lack G, Guest JF, J Med Econ 2010;13:119-128
You may also be interested in
Help us provide information most relevant to you
Please ensure your role and areas of interest are up to date.
Also on this website
About Nutricia
Follow us on LinkedIn
Follow us on Twitter
- Nutricia Ireland Limited is a company registered in the Republic of Ireland with company number 106997. VAT Number IE4800652P
- © 2024 Nutricia. All rights reserved